


MedLine
Artnovion Healthcare
COVID Safe Acoustics
Healthcare & Well-being product line by Artnovion
Healthcare and Well-being facilities are two very particular environments where noise problems have the potential to become major determinants of service quality.
In this paper we review the need for acoustical treatment in Healthcare and Well-being environments and explore the particular demands of hospital settings.
Artnovion has develop an antimicrobial and sterilizable product line specifically designed to meet the high standards of infection control and face the challenges of the Covid-19 pandemic.
This paper explains the technology behind these products.
The Well-being sector
Well-being spaces offer restful and peaceful environments in order to make customers experience more pleasant and enjoyable.
Acoustic quality in this kind of space is a base requirement.
However, due to the often highly humid environments, this kind of facility has particular characteristics and requirements that demand for more specific solutions.
While some areas (atriums, waiting rooms or corridors) will require only standard acoustic treatment solutions, other spaces (like changing rooms, locker rooms, gyms, pools, jacuzzi, saunas or massage rooms) will greatly benefit from acoustic treatment solutions that also offer additional features such as odour control, mould control and have cleanable or antimicrobial surfaces.
It's all about treating noise in a healthy way.

Healthcare facilities

But when it comes to healthcare facilities, the stakes are much higher. Acoustic levels in hospitals are very high and have been growing significantly since 1960. On average, daytime noise levels have risen 0,38 dB and nighttime levels have risen 0,42 dB each year. (I. Busch-Vishniac, 2005) The sources of noise are multifold and are both internal and external. Internal noise coming from bedside life support systems, infusion pumps, incubators, multiple monitors and alarms adds to the external noise from cooling systems, emergency generators, often construction or renovation works, along with constant ambulance sirens or nearby public transport. (Aurélio & Tochetto, 2010)
Furthermore, the noise generated by the hospital staff, the communication and circulation of patients, patient care teams and families contribute to the epidemic of noise in healthcare, which factors as one of the biggest complaints of both patients and staff.
Regardless of where the patient is, noise generated by equipment and other people tend to dominate the hospital's acoustical experience.
Acoustics impact perceptions of privacy, comfort, safety, and security for patients and their families. (Acoustics in Healthcare Environments, 2010)
The consequences of noise on hospitalized patients is well documented and has a negative impact on a patient's physiological health, increasing their chances of being readmitted to the hospital. (I. Hagerman, 2005) Depending on the condition of the patient and the level of care, poor acoustical conditions may impact recovery and healing processes in different ways.
In a physiological response to noise, adult patients in a general ward can experience startle reflexes, increased blood pressure and higher respiratory rates which may lead to irritation, impaired pain tolerance, confusion, irritation and delirium. (Claudia Giliberti, 2015) Noise can also cause significant sleep disruption, which is also closely associated with cardiovascular stress, impaired immune function and catabolic metabolism.
These effects are particularly significant in Intensive Care Units (ICU) where noise has been reported to be associated with a greater requirement for sedation and anesthesia. (Avinash Konkani, 2012)
The healthcare environment where noise is potentially the more deleterious is the Neonatal Intensive Care Unit (NICU). Besides the cardiovascular effects that are well documented for adults, newborn or premature babies are more vulnerable to acoustic stimuli.
In these patients, noise has been associated with more serious consequences, such as apnea, hypoxemia, the elevation of cranial pressure and modulation of neuroendocrine and immune systems. (B. H. Morris, 2000) (E. M. Wachman, 2011)
In these patients, stress responses may increase the risk of adverse effects like growth impairment, auditive deficits, retinopathy, and affect many other early development processes. (A. Almadhoob, 2015) Parental communication with newborns, namely the ability of the baby to recognize and relate to the mother's voice, is fundamental for attachment processes, and is also affected by surrounding noise, leading to disruption to the baby's wellbeing. (Vera Santos, 2018)
Besides the effect on patients, high noise levels also affect healthcare professionals, contributing to distraction and memory loss which may lead to accidents and errors. (M. Shahheidari, 2012)
Speech intelligibility and privacy issues are other significant concerns for healthcare environments where clear communication between professionals and patients is paramount. (Acoustics in Healthcare Environments, 2010)
For all the above reasons, the World Health Organization (WHO) has developed guidelines for noise in healthcare facilities where nighttime noise should not exceed 40 dB (LAmax). For inpatient wards, the recommended interior noise level is 30 dB LAeq during daytime and 35 dB LAeq at night. (Taskforce, April 1999). In 1997, the American Academy of Pediatrics established that noise levels higher than 45 dB should not be admitted in a NICU setting. (American Academy of Pediatrics, 1997)
Despite abundant evidence and recommendations, virtually no healthcare facility has yet been able to meet these standards. Instead, the acoustic reality in most of the studied sites is still so far away from these values that some authors have suggested the definition of more realistic noise control objectives. (Darbyshire, 2016)

Particular concerns for healthcare facilities
Acoustical treatment in healthcare facilities needs to take in to account particular concerns related to infection control.
The incidence of Hospital-Acquired Infections (HAIs), also known as nosocomial infections has been growing exponentially since 1980 due to the emergence of multidrug-resistant bacteria microorganisms. (A. C. Abreu, 2013)
These are infections that occur in patients in a hospital or healthcare facility which were not present at the time of admission, including infections that are acquired in the hospital but are diagnosed only after discharge.
Patients and patient care teams carry pathogens on their hands resulting from direct contact with other infected patients or colonized surfaces. Once patients or surfaces become contaminated, they act as a reservoir for infectious bacteria. (Collins, April 2008) Environmental contamination can persist for many days and months with several pathogens, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), norovirus and Clostridium difficile (C. difficile). (Sehmi, 2016)
Besides regular scheduled cleaning and disinfection of hospital equipment and surfaces, (including alternative methods that go beyond basic cleaning), many other strategies have been adopted for controlling nosocomial infections. (Sehmi, 2016)
A promising component of these strategies is the use of antimicrobial surfaces that prevent microorganism adhesion and can reduce microbial burden without staff having to spend hours manually cleaning surfaces. (Kristopher Page, 2009)
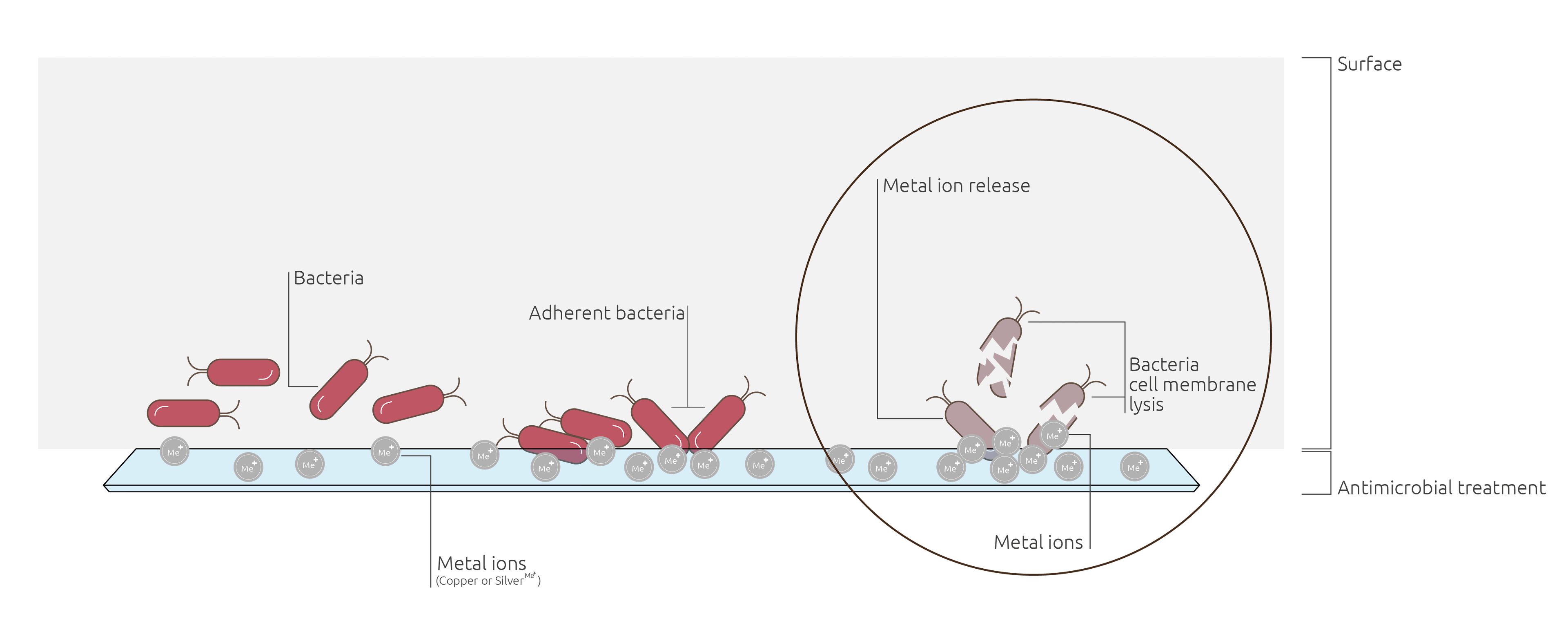
There are several options available to give antimicrobial properties to hospital surfaces. One of the most effective methods consists in using metal ions (Copper or Silver) which have the well-documented ability to break down bacterial cell walls, resulting in microbicidal and sporicidal activity. (Otter, 2014)
These ions can be embedded in surface coatings that convey both antimicrobial and antifungal properties.
Bacteria are also responsible for the producing scent molecules that cause unpleasant odors, so another significant result of the bactericide action of these coatings is an anti-odor effect. (Chakraborty, 2015) A treated surface or coatings will have lasting anti-odor properties.
The metal ions can also be incorporated into textiles, conveying to fabrics the same antimicrobial properties. (Diana Santos Morais,2016) Studies have demonstrated that Silver and copper ions remain bonded to the fabric fibers in a durable way that can resists multiple washings. (Oguz Demiryurek, 2019)
Metal Ion Antimicrobial Mechanism
The Challenge of COVID-19
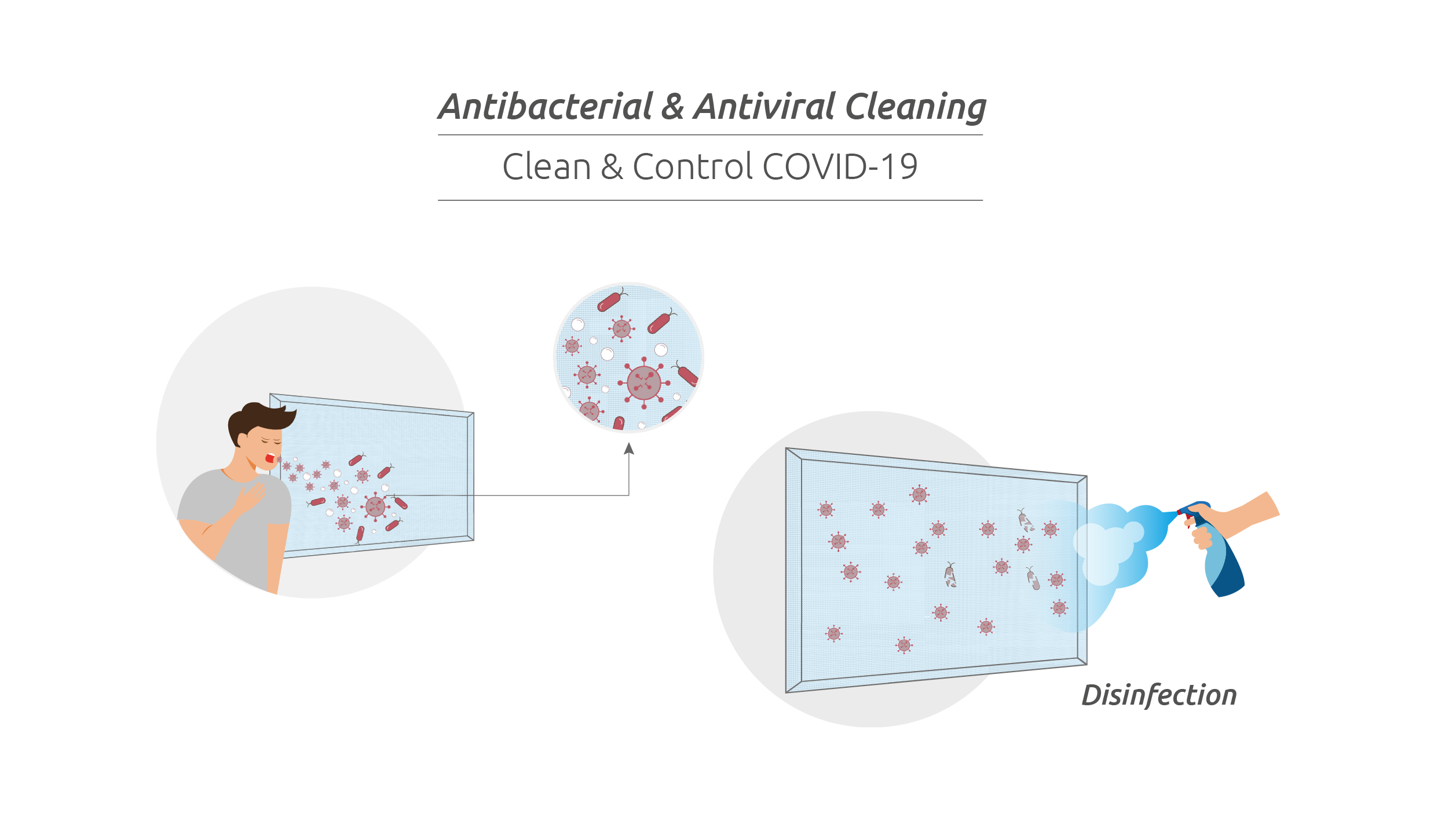
The recent pandemic of Coronavirus disease 2019 (COVID-19) - a respiratory infection caused by SARS-CoV-2 (COVID-19 virus) - has changed the landscape regarding standard approaches to healthcare infection control.
This virus, which is transmitted mainly through close physical contact and respiratory droplets, has also been reported to have airborne transmission during aerosol generating medical procedures. Despite the still limited evidence regarding effective infection transmission through surface contamination, the infection prevention and control principles (namely cleaning and disinfection practices) designed to mitigate the spread of pathogens and to limit the role of fomite transmission in healthcare settings, are currently recommended by the World Health Organization. (World Health Organization, 2020)
Compared to bacteria and fungi, viruses present a different challenge as they do not proliferate by themselves on inert surfaces. Instead, viruses rest on surfaces waiting for a new host to inadvertently touch that surface and carry them to contact with any mucosa, where they will infect the host and use the host's cells to replicate and to thrive.
SARS-Cov-2 is, like other coronaviruses, an enveloped virus with a fragile outer lipid envelope that makes it more susceptible to disinfectants when compared to non-enveloped viruses. (Rutala, 2019) For this reason, besides the regular antimicrobial protection, the best way to defend against the new COVID-19 threat, is to regularly clean all the exposed surfaces with disinfectant products.
The selection of disinfectants should take into account the targeted microorganisms, as well as the recommended concentration and contact times, according to the manufacturer's instructions. Hypochlorite based products, which include liquid or solid formulations are amongst the most frequently used solutions in hospital settings. Spraying or fogging solutions are not recommended. (World Health Organization, 2020).
A list of disinfectants for use against the COVID-19 virus is currently being actively updated by the U.S. Environmental Protection Agency (EPA). (Environmental Protection Agency, s.d.)
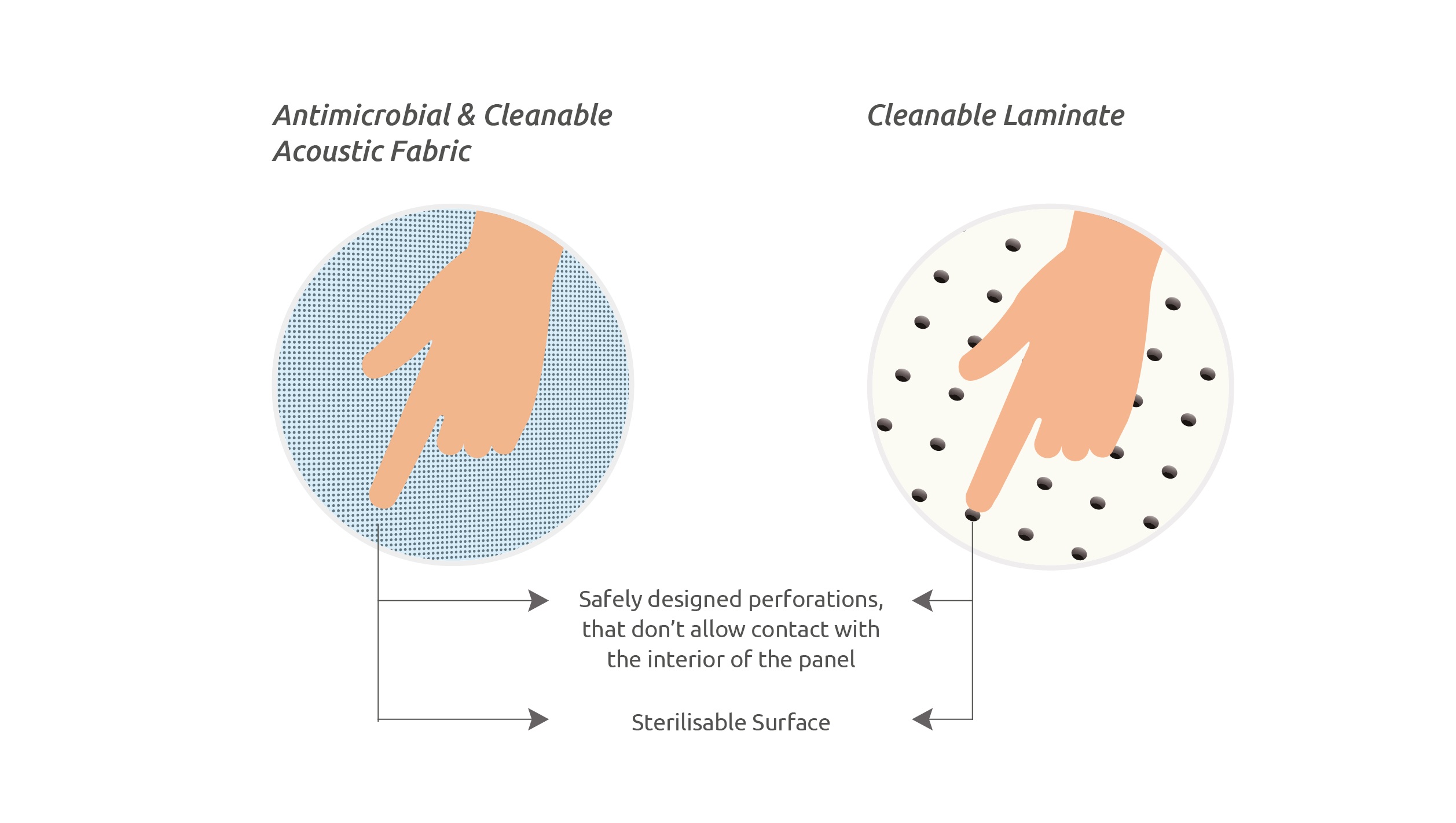
The surfaces of any hospital acoustical treatment equipment need therefore to both have antimicrobial properties and endure thorough and regular cleaning.
The surfaces of acoustical equipment need to be perforated, allowing for sound waves to penetrate the panel for optimal sound absorption.
This poses the question of the potential contamination of the inner surface inside the perforations.
In what regards the possibility of infection transmission, surface resting pathogens – either viruses or other microorganisms - can only be carried by direct contact with a new host.
As the outer surface is both antimicrobial (not allowing for microorganism growth) and also regularly disinfected, the perforation holes do not contribute to infection transmission as the inner perforation surfaces cannot be touched.
While in public and open access areas noise level can be managed with standard products as in any other public building in restricted inpatient areas, the need for acoustical treatment incorporating cleanable or antimicrobial surfaces becomes increasingly more significant, as the level of care grows for each type of space.
The problem of Hospital-Acquired Infections has also led to the creation of infection control teams dedicated to address any aspect of hospital life which may result in increased risk of infection transmission or in further growth of drug resistances.
Amongst many other tasks, these teams are called to analyze and approve all aspects of infection control related to any new equipment that may need to be installed for acoustic treatment.
In conclusion, there is therefore an obvious demand for acoustic treatment for well-being healthcare facilities. In this context, acoustic equipment needs to deliver both effective noise control and infection control properties, by presenting antimicrobial properties and enduring thorough and regular cleaning.
Bibliography
A. Almadhoob, A. O. (2015). Sound reduction management in the neonatal intensive care unit for preterm or very low birth weight infants. 2015,. Obtido de Cochrane Database of Systematic Reviews: Issue 1. Art. No.: CD010333
A. C. Abreu, R. R. (2013). Current and emergent strategies for disinfection of hospital environments. Journal of Antimicrobial Chemotherapy., pp. 1-15. (2010). Acoustics in Healthcare Environments. Ceilings & Interior Systems Construction Association.
American Academy of Pediatrics. (1997). Noise: A Hazard for the Fetus and Newborn. Pediatrics, 100 (4), pp. 724-727.
Aurélio, F. S., & Tochetto, T. M. (2010). Mensuração do ruído em uma Unidade de Terapia Intensiva Neonatal. Acta Pediátrica Portuguesa, 41(2), 64-68.
Avinash Konkani, B. O. (2012). Noise in hospital intensive care units — a critical review of a critical topic. Journal of Critical Care, 27.
B. H. Morris, M. K. (2000). The full-term and premature newborn – Physiological effects of sound on the newborn. Journal of perinatology, 20, pp. S54-S59.
Carlos Oliveira, G. A. (2012). Occupational Exposure to Noise Pollution in Anesthesiology. Rev Bras Anestesiol, 62 (2), pp. 253-261.
Chakraborty, G. D. (2015). Antimicrobial performance of cotton finished with triclosan, silver and chitosan. Fashion and Textiles, 2-13.
Claudia Giliberti, R. M. (2015). Noise in Healthcare Facilities. 22nd International Congress on Sound and Vibration. Florence.
Collins, A. S. (April 2008). Preventing Health Care– Associated Infections. Em R. G. Hughes, Patient Safety and Quality: An Evidence-Based Handbook for Nurses. (p. Chapter 41). Rockville : Agency for Healthcare Research and Quality (US);.
Darbyshire, J. L. (2016). Excessive noise in intensive care units Bad for staff and very bad for patients. BMJ, p. 353.
Diana Santos Morais, R. M. (9 de 2016). Antimicrobial Approaches for Textiles: From Research to Market. Materials, p. 498.
E. M. Wachman, A. L. (2011). The effects of noise on preterm infants in the NICU. Arch Dis Child Fetal Neonatal, 96, pp. F305–F309.
Environmental Protection Agency. (n.d.). List N: Disinfectants for Use Against SARS-Cov-2 (COVID-19). Retrieved from Pesticide Registration: https://www.epa.gov/pesticide-registration/list-n-disinfectants-use-against-sars-cov-2
I. Busch-Vishniac, J. W. (2005). Noise levels in Johns Hopkins Hospital. Journal of the Acoustical Society of America, 118 (6), 3629–3645.
I. Hagerman, G. R. (2005). Influence of intensive coronary care acoustics on the quality of care and physiological state of patients. International Journal of Cardiology, 98 (2), 267–270.
Kristopher Page, M. W. (2009). Antimicrobial surfaces and their potential in reducing the role of the inanimate environment in the incidence of hospital-acquired infections. Journal of Materials Chemistry, 19, 3819– 3831.
M. Shahheidari, C. H. (2012). Impact of the design of neonatal intensive care units on neonates, staff, and families: a systematic literature review. J Perinat Neonatal Nurs., 26 (3), pp. 260-266.
Oguz Demiryurek, T. T. (2019). Antibacterial Activity and Durability of some Regenerated Cellulosic Fabrics Treated with Zn, Cu and Ag Metal Salts After Repeated Laundering. Cellulose Chemistry and Technology, 53 (1- 2), 163-173.
Otter, J. (12 de February de 2014). An overview of the options for antimicrobial surfaces in hospitals. Taken from REFLECTIONS ON INFECTION PREVENTION AND CONTROL
Rutala, W. W. (2019, 01 14). Best practices for disinfection of noncritical environmental surfaces and equipment in health care facilities: A bundle approach. . Am J Infect Control , 47, pp. A96–A105.
Sehmi, S. K. (2016). Antibacterial Surfaces with Nanoparticle Incorporation for Prevention of Hospital- Acquired Infections. Thesis (Doctoral). University College London.
Taskforce, E. (April 1999). Guidelines for community noise – Report on the expert task force meeting. London (United Kingdom): Word Health Organization.
Vera Santos, E. S. (2018). Consenso Clínico - “O Som na Unidade de Neonatologia”. Sociedade Portuguesa de Neonatologia.
World Health Organization. (2020, 05 15). Cleaning and desinfection of environmental surfaces in the context of COVID-19. Interim guidance. WHO.